
How much is too much when it comes to cryoablation volumes in solitary kidneys?
Percutaneous cryoablation of small kidney masses is preferred by many providers due to the procedure’s renal function-sparing capabilities. However, it is not without risks, especially in patients with only one kidney.
A paper in the Journal of Vascular and Interventional Radiology offers new guidance on how ablation volumes affect renal function in solitary kidneys and highlights ranges that pose the least risk to patients.
“Treatment of renal lesions in patients with a solitary kidney requires extra consideration,” corresponding author Charles Y Kim, MD, from the division of interventional radiology at Duke University Medical Center, and colleagues suggested. “Thus, strategies for maximal nephron-sparing are needed to prolong renal function and minimize risk of end-stage renal disease.”
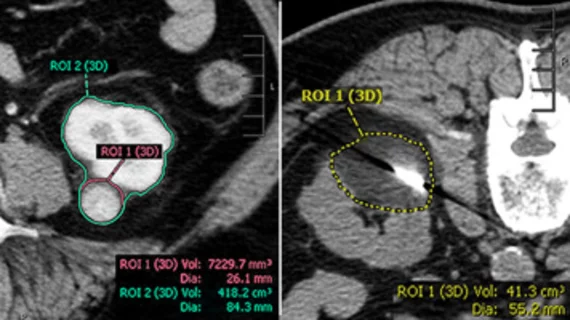
Cryoablation is known to be a nephron-sparing approach; however, it does have limitations. To better define them, researchers analyzed all cryoablation procedures conducted on solitary kidneys at a single facility over a 15-year period. Post-cryoablation renal function was based on the lowest serum creatinine within six months of the procedure, while alterations in function were determined using glomerular filtration rate (GFR) changes. These metrics were compared alongside a volumetric analysis performed on target lesions, renal parenchyma and ablation zones.
At baseline, all patients had stage 2 or worse chronic kidney disease (CKD). On average, patients who underwent cryoablation had an 8% decrease in GFR at the median follow-up of 95 days.
Any decreases were found to be closely associated with parenchymal ablation volume. The median volume of ablated parenchyma was 19.7mL, or around 8.1% of total parenchyma. However, only moderate reductions in renal function were observed in ablations of up to 20% of total parenchymal volume, the group noted.
None of the patients developed end stage renal disease within one year of their procedure, even those who underwent more aggressive ablations. What's more, comorbidities like diabetes and hypertension—both known to further deteriorate renal function—also did not contribute to deteriorations in function.
“Patients with CKD might be expected to be at higher risk of major renal decline after losing parenchymal volume with renal cryoablation. However, no significant correlation was found between baseline renal function and post-ablation renal function change,” the group wrote, adding that ablation of 20% normal renal parenchyma in a solitary kidney could be considered “a reasonably safe threshold.”
The study abstract is available here.

In addition to her background in journalism, Hannah also has patient-facing experience in clinical settings, having spent more than 12 years working as a registered rad tech. She began covering the medical imaging industry for Innovate Healthcare in 2021.